When a pharmaceutical brand invests millions into digital advertising, they’re ultimately asking one question: did this campaign change prescribing behavior? In healthcare, that answer is genuinely difficult to get.
Unlike consumer marketing, where a click can quickly lead to a purchase, healthcare decisions unfold over weeks or months and across disconnected systems. Ads are served in one environment, website visits happen in another, and prescriptions appear later in claims data. Most attribution models weren’t designed with that kind of timeline in mind.
At Wrango, we built an attribution system specifically for healthcare. The goal was to go beyond connecting impressions to clicks, and instead connect exposure to real-world prescribing outcomes.
Why Healthcare Attribution Breaks Down
There are three characteristics of healthcare that standard attribution tools tend to struggle with.
Shared environments. Hospitals and large practices often route many clinicians through the same networks. This makes IP-based attribution unreliable on its own, since a single IP address can represent hundreds of different providers.
Long decision cycles. A physician may encounter an ad today, visit a product site weeks later, and write a prescription months after that. Short attribution windows are not a great fit for a decision process that unfolds over that kind of timeframe.
Privacy requirements. Healthcare data requires careful handling and user consent, which shapes how identity can be captured and resolved. Tools built for consumer contexts often don’t translate cleanly here.
These aren’t edge cases. They’re the norm in healthcare, and any measurement approach needs to account for them.
A Layered Approach to Identity and Outcomes
Rather than relying on a single signal, Wrango combines multiple layers, each designed with these healthcare-specific constraints in mind.
The first layer uses deterministic device identifiers and email-authenticated events that can be resolved to individual healthcare providers. Where this is possible, it gives us high-confidence matches for known audiences.
Where direct identity resolution isn’t available, we use behavioral signals that connect website visits back to prior ad exposures. This happens within a scoped and controlled context, limited to the correct brand and pixel, which helps keep false positives low.
The third layer is prescription claims data paired with control groups. For every provider who was exposed to a campaign, we compare their prescribing behavior against a matched peer who wasn’t. This is what moves measurement from correlation toward something closer to causation.
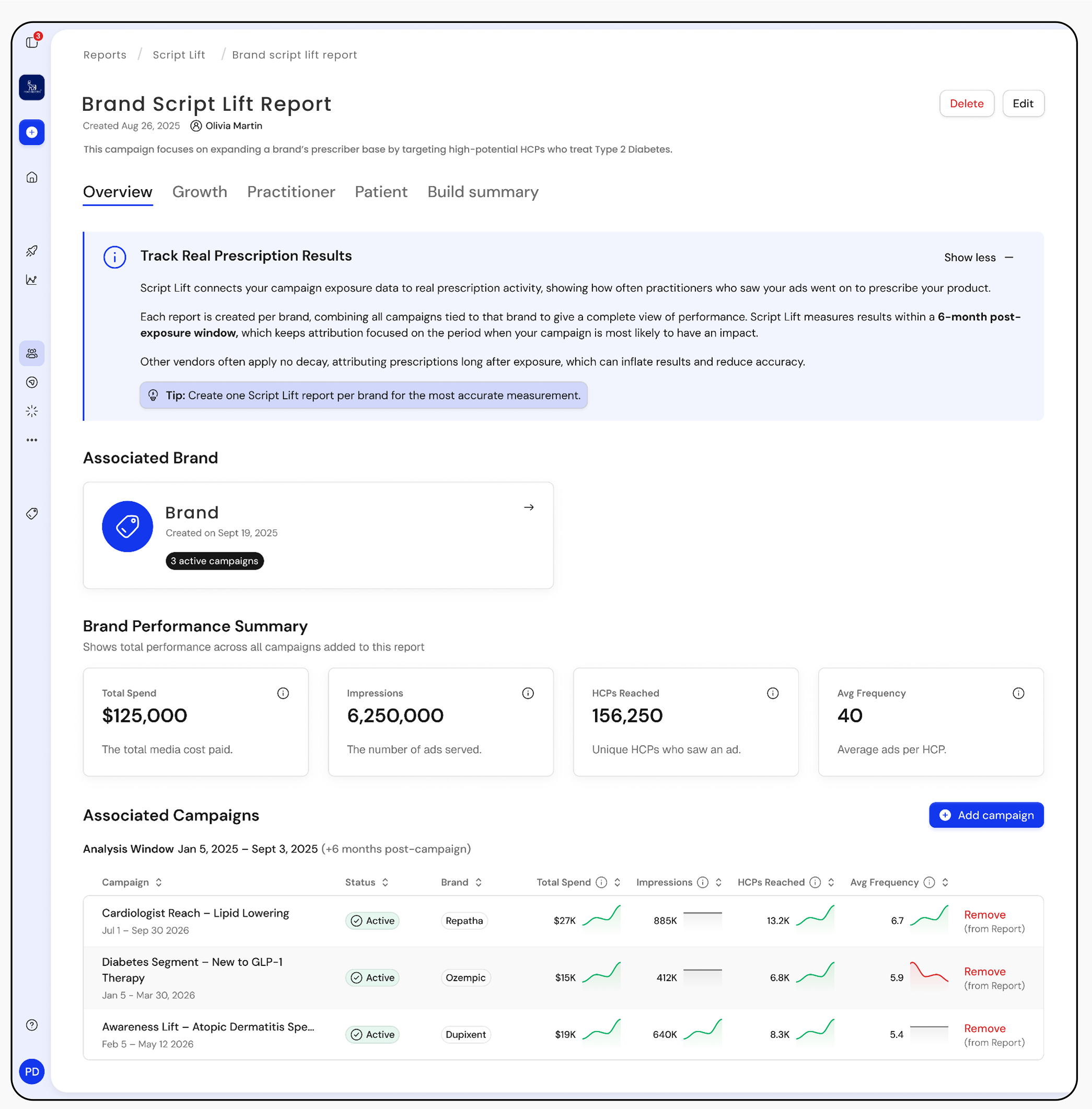
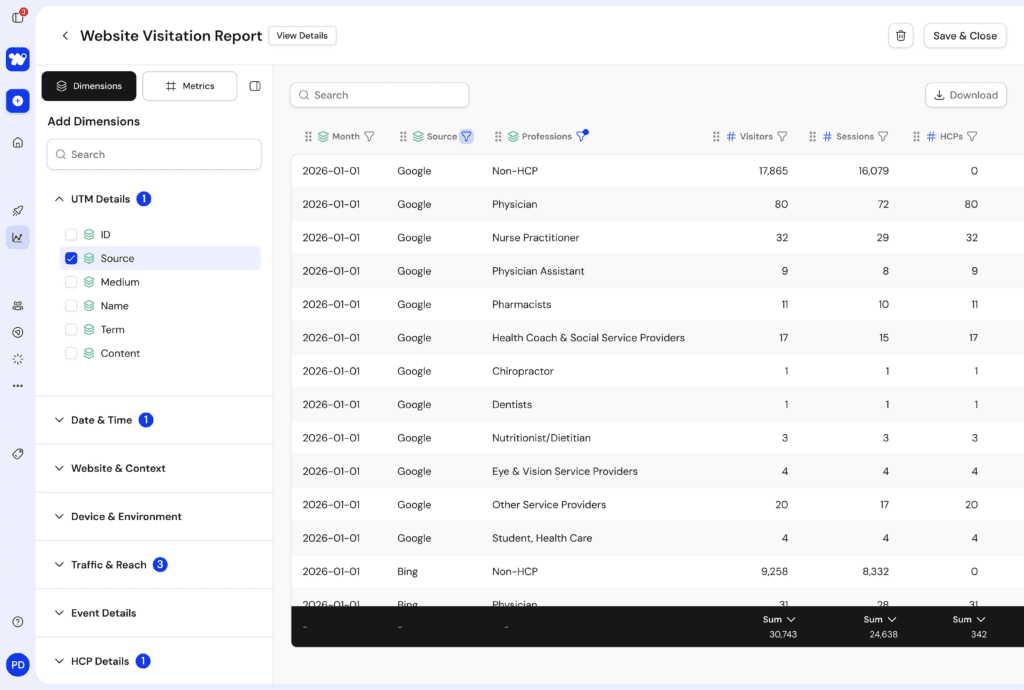
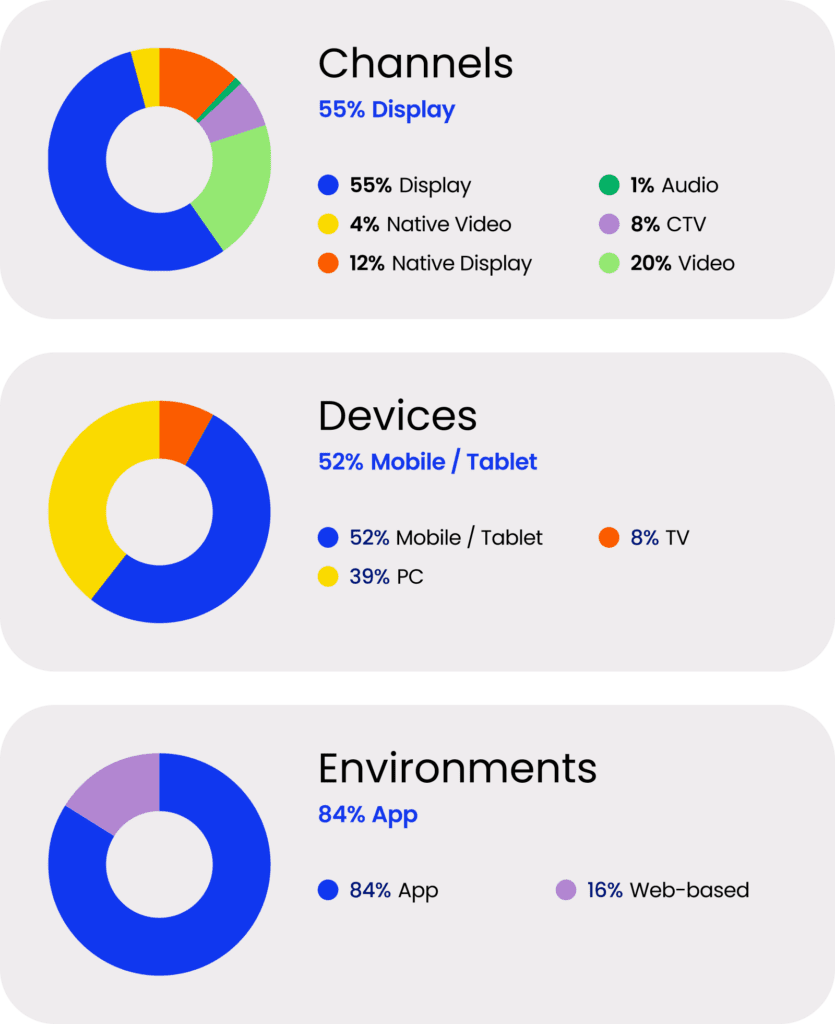
All campaigns, all DSPs, one report. Wrango’s Script Lift view consolidates exposure across every linked campaign into a single brand-level picture, with an attribution window built to reflect how healthcare decisions actually unfold.
Healthcare campaigns typically run across multiple platforms, which creates a practical challenge: stitching together reports from different DSPs makes it hard to deduplicate reach, compare performance consistently, or see the full picture in one place.
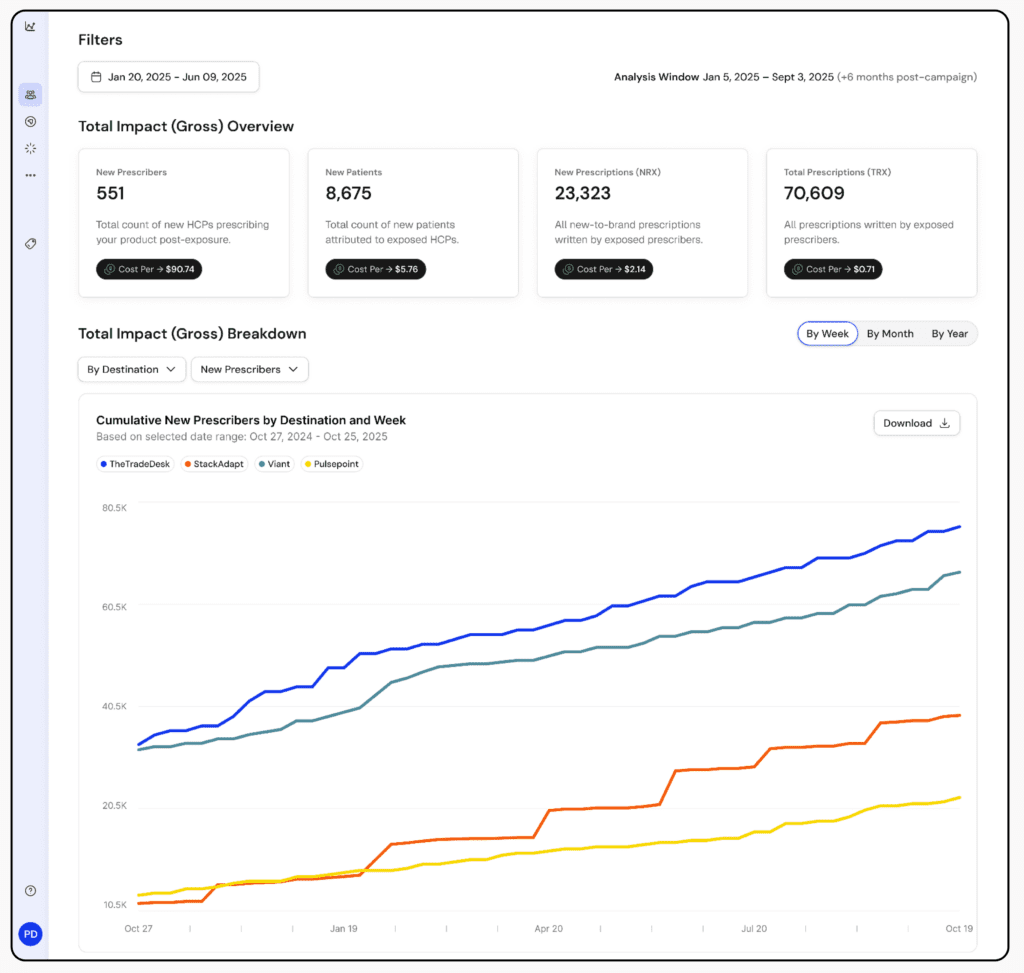
New prescribers tracked cumulatively across DSPs are deduplicated across all campaigns linked to a single report.
Measuring What Actually Matters
Attribution tells you who saw an ad. Lift measurement tells you whether the campaign had any effect on behavior isolated from everything else your brand is doing to convert prescribers. They’re related but distinct questions.
The reason the distinction matters is that without a control group, it’s easy to overestimate impact. If a campaign reaches physicians who were already likely to prescribe, the numbers can look strong even if the advertising had no real influence. Comparing against a matched unexposed group is what makes it possible to separate genuine lift from background prescribing patterns.
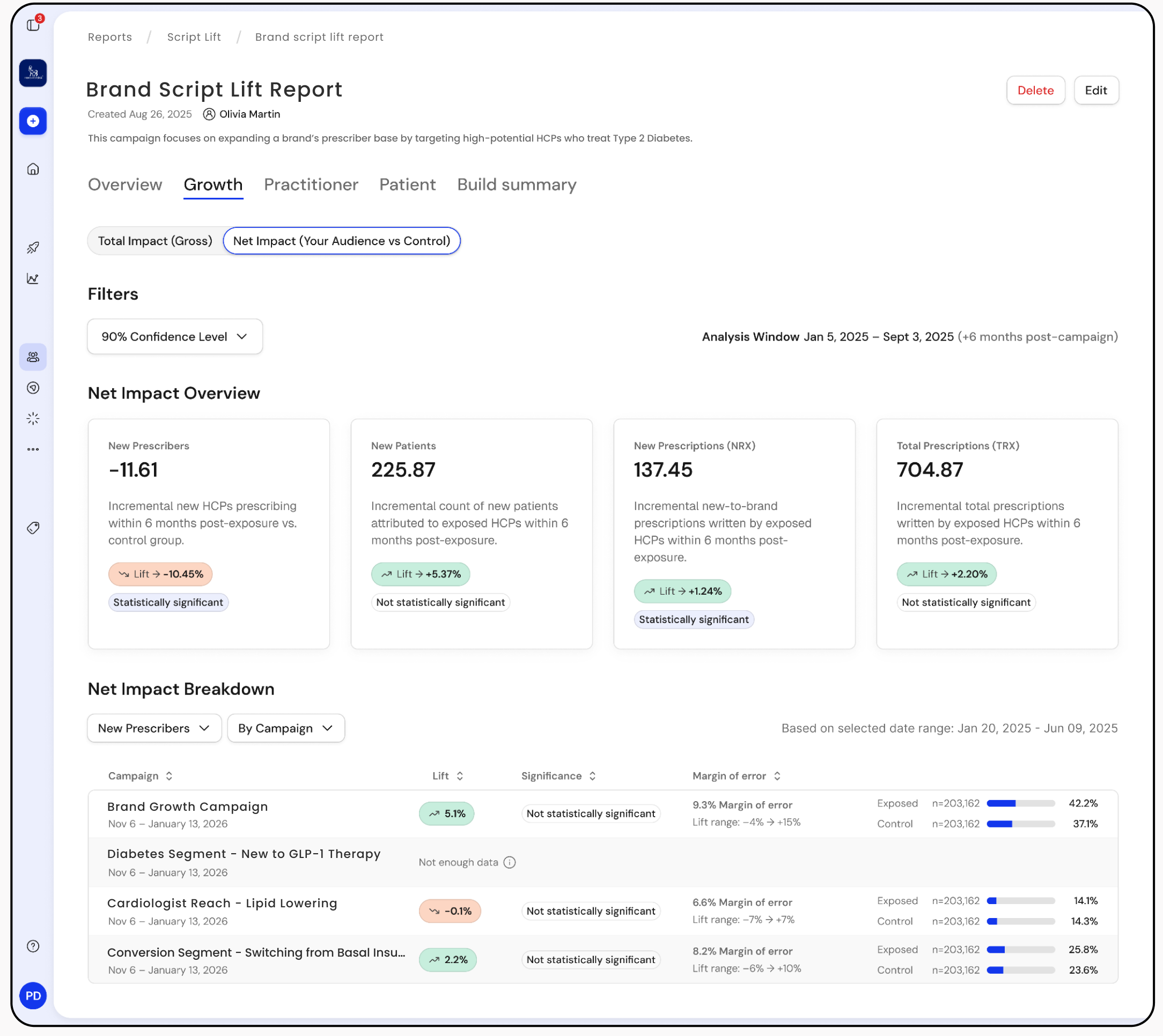
Did the campaign change prescribing behavior? Wrango’s Script Lift report compares exposed physicians against a matched peer group to show the real difference the campaign made.
Healthcare marketers deserve the same quality of measurement that consumer brands have come to expect, adapted for healthcare’s longer timelines, data requirements, and regulatory environment.
The Takeaway
Measuring campaign impact in healthcare requires infrastructure built for:
- Long decision cycles
- Shared clinical environments
- Strict privacy standards
- Real-world prescription validation
Getting to a reliable answer on prescribing lift takes more than a standard attribution model. It takes a system designed around how healthcare actually works. That’s what we focused on building at Wrango.
Learn More
If you’re evaluating how your campaigns measure prescribing lift, it may be time to rethink whether your attribution model reflects healthcare’s realities.
Connect with our team to learn how Wrango measures exposure, lift, and outcomes.